If you have been suffering from chronic heel pain, you have likely been told you have Plantar Fasciitis. You may have tried stretching, icing, special insoles, and rest, only to find that the burning pain in your heel just won’t go away.
If this sounds familiar, you might not have a muscle or tendon problem at all. You might have a pinched nerve.
This specific condition is called Baxter’s Neuropathy, and it is one of the most common—yet frequently misdiagnosed—causes of persistent heel pain. Here is everything you need to know about what it is, how to tell it apart from other foot problems, and how we actually diagnose it.
What is Baxter’s Neuropathy?
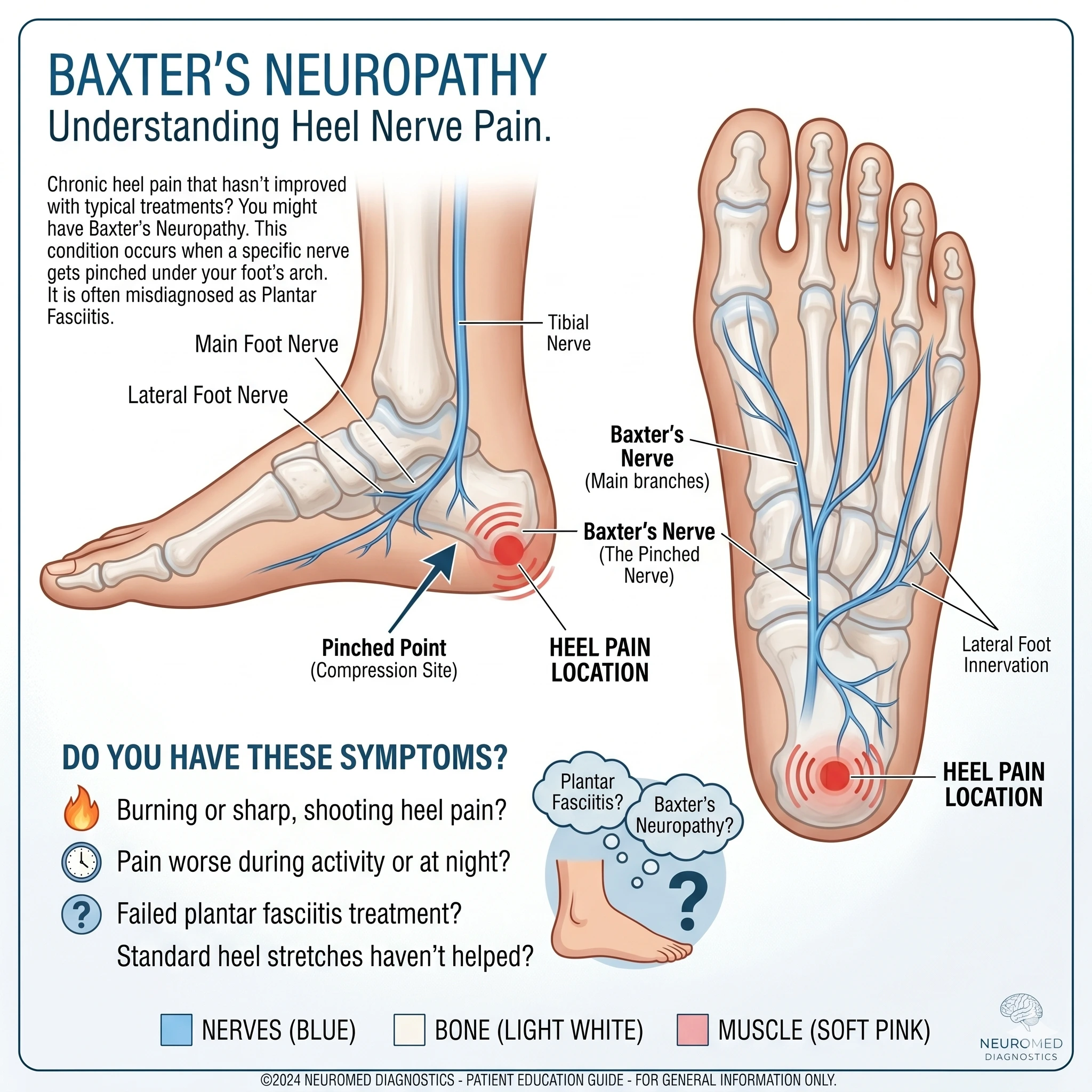
Baxter’s Neuropathy is the compression or “pinching” of a specific nerve in your foot called the inferior calcaneal nerve (often referred to as Baxter’s nerve).
As the nerves travel down your leg and into your foot, they pass through tight spaces. Baxter’s nerve branches off and travels directly under the heel bone. Because of its location, it is highly vulnerable to becoming trapped or compressed between the tight muscles and fascia of the sole of your foot. When this nerve gets pinched, it sends continuous pain signals right to your heel.
Is it the same as Tarsal Tunnel Syndrome?
No, though they are close neighbors! Tarsal Tunnel Syndrome involves a larger “parent” nerve (the posterior tibial nerve) getting trapped higher up, near the inside of your ankle. Tarsal Tunnel usually causes broad numbness, tingling, and burning across the entire bottom of the foot and toes.
Baxter’s Neuropathy happens further down the line and focuses the pain intensely on the bottom and inside of the heel.
What Causes Baxter’s Nerve to Get Trapped?
You might be wondering, “Why did this happen to me?” Baxter’s Neuropathy usually develops from mechanical pressure on the foot. The most common risk factors include:
Flat Feet (Overpronation): When your foot rolls inward too much, it pulls the fascia tight directly over the nerve.
Heel Spurs: A bone spur on the heel can physically press against the nerve.
Obesity or Sudden Weight Gain: Extra weight increases the downward pressure on the arches and nerves.
High-Impact Activities: Running or sports that require repetitive jumping on hard surfaces.
Prior Injuries: A history of bad ankle sprains can alter your foot biomechanics, putting new stress on the heel area.
Plantar Fasciitis vs. Baxter’s Neuropathy: How to Tell the Difference
Because both conditions cause intense heel pain, up to 20% of chronic plantar fasciitis cases are actually suspected to be Baxter’s Neuropathy. Here is how the symptoms typically differ:
Signs it might be Plantar Fasciitis:
Pain is usually worst with the very first steps in the morning.
The pain often lessens as you walk around and “warm up” the foot.
The pain is a deep ache or stabbing sensation.
Signs it might be Baxter’s Neuropathy:
The pain often gets worse the longer you are on your feet or as the day goes on.
The pain is frequently described as burning, sharp, shooting, or radiating.
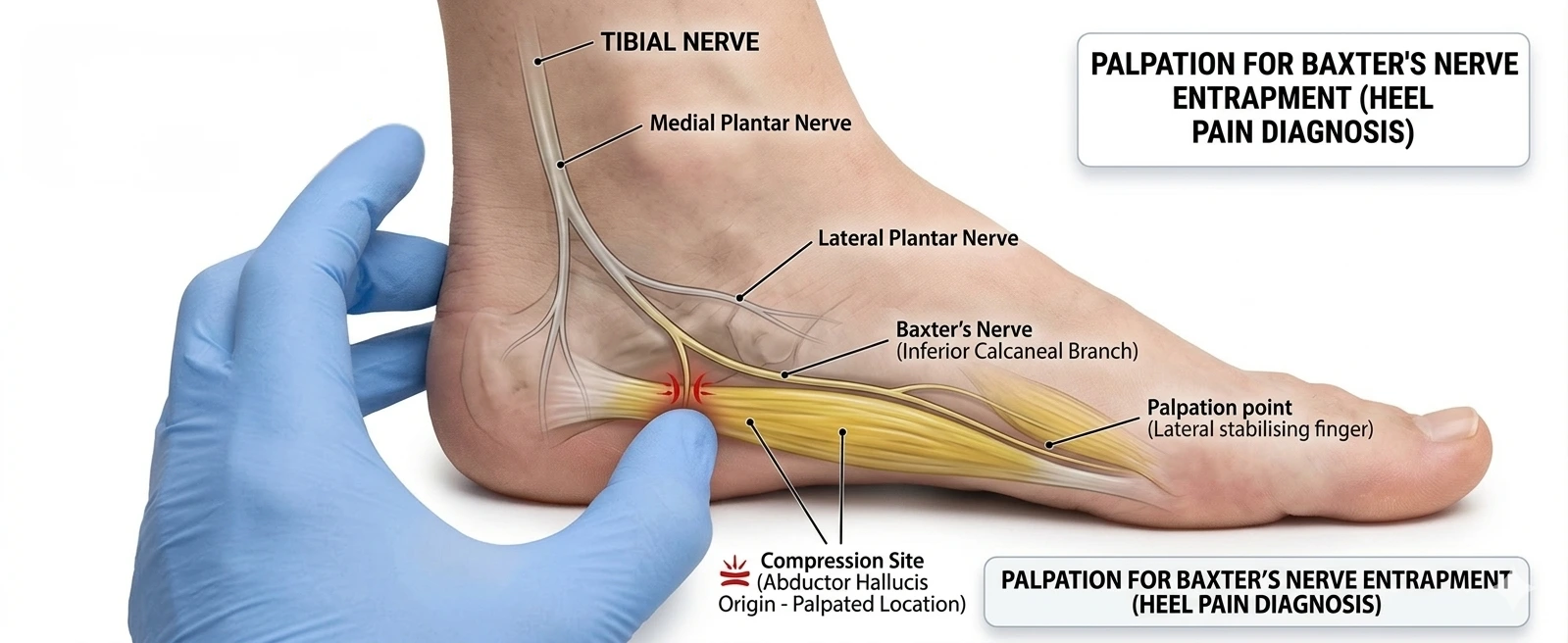
Pressing on the inside of the heel (where the nerve runs) reproduces the shooting pain.
You may experience numbness or tingling around the heel.
Standard treatments for plantar fasciitis (like stretching or splints) do not provide relief and might even make the burning worse.
How Do We Actually Diagnose It?
While an MRI or ultrasound can sometimes show swollen muscles or a thickened plantar fascia pressing on the nerve, imaging alone cannot definitively prove how well the nerve is functioning.
To find out exactly what is happening, we use specialized nerve tests. As a neurophysiologist, I use Electromyography (EMG) and Nerve Conduction Studies (NCS) to get a clear answer.
Here is how it works: Because Baxter’s nerve supplies power to a very specific muscle on the outside of your foot (the abductor digiti minimi), we can test that exact muscle. By measuring the electrical signals traveling through the nerve and into the muscle, we can clearly see if the nerve is trapped, delayed, or damaged. This test removes the guesswork and definitively separates a nerve entrapment from a simple tendon issue.
Treatment Options for Baxter’s Nerve Entrapment
Once accurately diagnosed, the goal is to take the pressure off the nerve.
Conservative Treatments:
Custom Orthotics: To support the arch and reduce tension on the tight fascia compressing the nerve.
Physical Therapy: Targeted at releasing the specific muscles (like the abductor hallucis) that wrap around the nerve.
Taping or Boot Bracing: To temporarily offload the heel.
Injections: A localized corticosteroid injection around the nerve can significantly reduce swelling and provide relief.
Proper Footwear (The “Best Shoes” Rule): Stop walking barefoot immediately! The best shoes for Baxter’s nerve entrapment have a deep, cushioned heel cup, rigid arch support (to stop the foot from rolling inward and stretching the nerve), and thick shock-absorbing soles. Avoid flat, unsupportive shoes like flip-flops or worn-out sneakers.
Surgical Treatments: If the nerve has been trapped for a long time and conservative methods fail, a minor surgical procedure called a surgical release may be necessary. A surgeon makes a small incision to release the tight fascia and muscle bands, freeing the nerve and eliminating the pain.
Frequently Asked Questions (FAQs)
Does Baxter’s Neuropathy go away on its own? Rarely. Because it is a mechanical entrapment (meaning something physical is squeezing the nerve), it usually requires intervention—like orthotics, injections, or targeted physical therapy—to remove the pressure. Ignoring it can lead to permanent nerve damage.
Can walking barefoot make Baxter’s Neuropathy worse? Yes. Walking barefoot removes all arch support and shock absorption, applying maximum tension and pressure directly to the bottom of the heel and the trapped nerve.
How long does it take to recover from Baxter’s nerve surgery? If a surgical release is needed, most patients can bear weight in a walking boot within a few days to a week. Full recovery and return to normal, high-impact activities typically takes about 4 to 6 weeks.
The Bottom Line: Stop Guessing and Get Tested
You do not have to live with heel pain forever. If you have been treating plantar fasciitis for months with no improvement, it is time to look at the nerves.
Don’t rely on guesswork. The most crucial step is finding a specialist who can accurately test the nerve’s function. Seek out a clinical neurophysiologist for an EMG/NCS test to get a definitive diagnosis. Once you know exactly which nerve is trapped, you can finally get the targeted treatment you need to walk pain-free again.
About the Author: Lead Editor, neuromedhub.com | Clinical Neurophysiologist