Every clinical neurophysiologist sees carpal tunnel syndrome (CTS) regularly—it is the bread and butter of electrodiagnostic medicine. During pregnancy, CTS is incredibly common, typically driven by hormonal shifts and fluid retention that lead to mild-to-moderate symptoms and classic electrophysiological slowing.
However, clinical neurophysiology is rarely a “one-size-fits-all” discipline. Every so often, a routine referral presents with findings that remind us why rigorous methodology matters. Atypical presentations—such as a subacute onset featuring a profound sensory conduction block—are less frequently highlighted in standard textbooks, yet they offer critical teaching points for accurate localization and prognostication.
In this clinical case study, we explore a real-world EMG presentation of pregnancy-related CTS with a bilateral sensory conduction block, emphasizing the methodology of segmental stimulation and the underlying pathophysiology of acute neurapraxia.
Case Presentation
A 27-year-old right-handed female, currently working as a school teacher, was referred to our electrodiagnostic laboratory for the evaluation of severe bilateral hand paresthesias.
She was in her 6th month of pregnancy (approximately 24–26 weeks of gestation). Her pregnancy had been uneventful up to this point, with standard gestational weight gain.
Medical History:
No history of diabetes mellitus, hypothyroidism, or rheumatologic disease.
No prior history of cervical radiculopathy or peripheral neuropathy.
No previous episodes of carpal tunnel syndrome prior to conception.
History of Present Illness: The patient reported a progressive, subacute onset of symptoms beginning during her 5th month of pregnancy. She described bilateral hand paresthesias strictly localized to the median nerve distribution. The symptoms were predominantly sensory, with severe nocturnal exacerbations that disrupted her sleep. She denied any gross motor weakness, dropping of objects, or proximal radiation of pain into the cervical spine.
Clinical Examination:
Motor: Preserved bulk in the thenar eminence with no visible atrophy. Abductor pollicis brevis (APB) strength was 5/5 bilaterally.
Sensory: Subjective altered sensation (hypoesthesia) over the palmar aspect of the first three digits.
Provocative Tests: Phalen’s maneuver and Tinel’s sign were both strongly positive bilaterally at the wrist.
Electrophysiological Evaluation
To thoroughly evaluate the extent of the compression and rule out a more diffuse polyneuropathy, a comprehensive nerve conduction study (NCS) was performed.
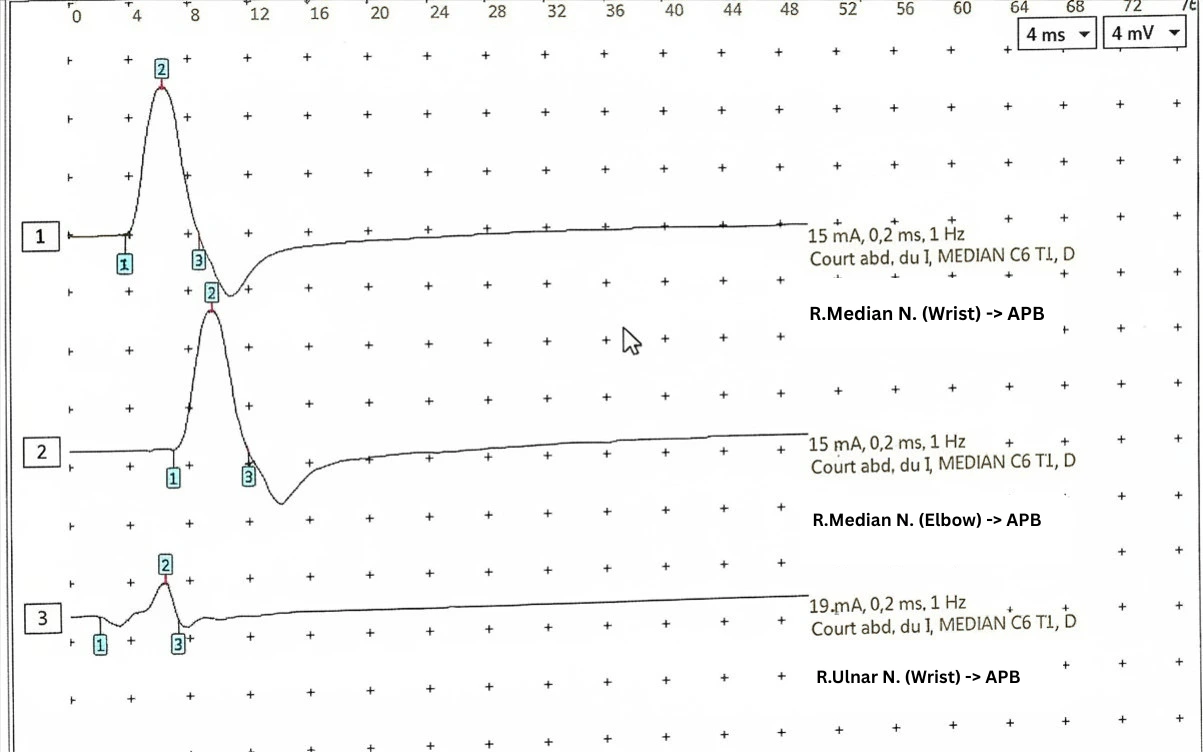
1. Motor Nerve Conduction Studies
The bilateral median nerves demonstrated prolonged distal motor latencies, consistent with slowing across the carpal tunnel. Crucially, the Compound Muscle Action Potential (CMAP) amplitudes recording the APB were robust and preserved, with no electrophysiological evidence of downstream motor axonal loss.
2. Sensory Nerve Conduction Studies (The Routine Approach)
A comparative sensory study between the median and ulnar nerves at the fourth digit (D4) was performed. This revealed significant latency differences and markedly reduced conduction velocities of the median nerve bilaterally, localizing a focal slowing to the wrist.
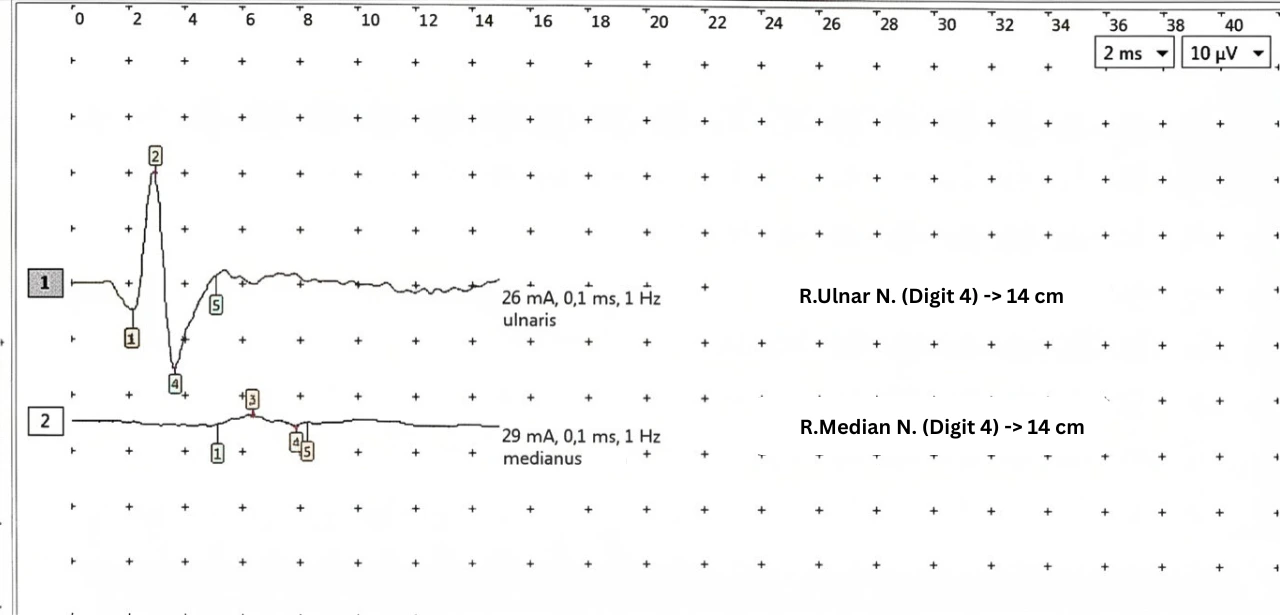
While this confirms a median neuropathy at the wrist, it does not fully explain the severity of her subacute sensory symptoms. To understand the true pathophysiology, a more rigorous methodological approach was required.
3. Advanced Electrophysiology: Segmental Stimulation
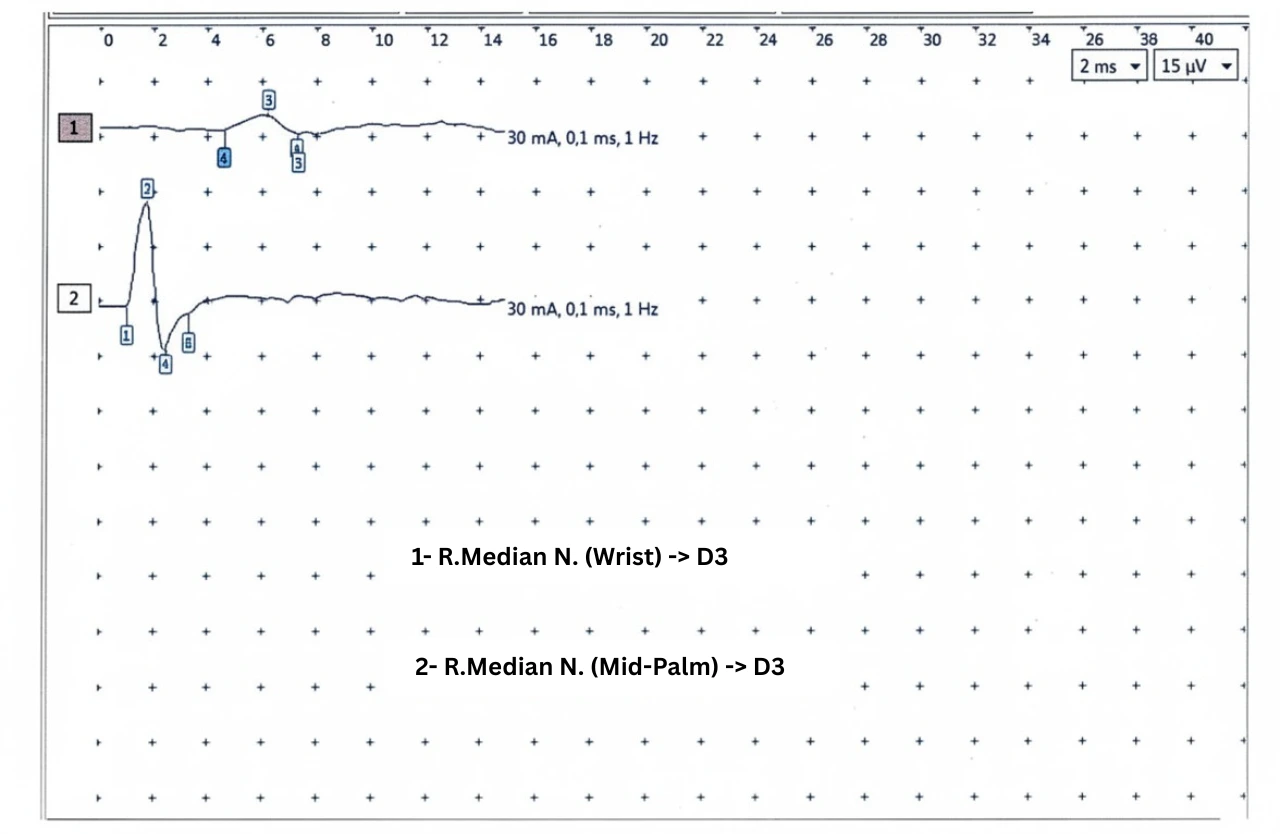
We proceeded with segmental sensory nerve conduction studies of the median nerve, recording at the third digit (D3). To accurately assess the nerve segment traversing the transverse carpal ligament, stimulation was performed precisely at both the mid-palm and the wrist.
The results revealed a dramatic sensory conduction block:
Mid-Palm Stimulation (Distal to the ligament): Robust Sensory Nerve Action Potential (SNAP) amplitudes of ~28–29 µV.
Wrist Stimulation (Proximal to the ligament): Precipitous drop in SNAP amplitudes to ~4–6 µV.
💡 Clinical Pearl: The 50% Rule for Demyelination
In clinical neurophysiology, an amplitude drop exceeding 50% across a short anatomical segment is the hallmark of a focal conduction block. In this patient, the palm-to-wrist amplitude drop was approximately 80% to 85%. Because the distal (palm) amplitudes were completely preserved, we can definitively diagnose a severe, localized neurapraxic lesion without significant distal axonal degeneration.
4. Definitive Diagnosis
Subacute bilateral pregnancy-related carpal tunnel syndrome with sensory conduction block.
Pathophysiology and Clinical Discussion
Most routine electrophysiological studies in pregnancy-related CTS report simple distal latency prolongation. This case highlights a critical, less commonly discussed feature: sensory conduction block can, and does, occur in subacute pregnancy-related CTS.
This profound focal demyelinating compressive neuropathy is driven by acute mechanical strangulation of the nerve. Rapid tissue edema and fluid retention within the confined space of the carpal tunnel “pinch” the myelin sheath, preventing the propagation of the action potential across the wrist.
However, because the axon itself remains intact (as evidenced by the healthy 28 µV SNAP obtained when stimulating distal to the compression at the palm), the distal nerve segment remains viable.
Why This Matters for Clinical Practice
Avoiding Misdiagnosis: If a practitioner only stimulates at the wrist and records a 4 µV SNAP, they might erroneously conclude the patient has severe axonal loss (Wallerian degeneration). By performing segmental stimulation at the palm, we unmask the conduction block and prove the axons are actually healthy.
Prognostication: A demyelinating conduction block (neurapraxia) carries a vastly superior prognosis compared to an axonal lesion.
Management and Prognosis
Because the electrophysiological data proved there was no irreversible axonal loss, the patient was reassured that her condition, while highly symptomatic, was benign and highly reversible.
Surgical intervention (carpal tunnel release) is rarely indicated during pregnancy and should be strictly avoided in cases of pure neurapraxia.
Treatment Plan:
First-line: Rigid nocturnal wrist splinting to maintain neutral alignment and maximize canal volume.
Prognosis: Excellent. The localized tissue edema is expected to resolve during the post-partum diuresis phase. Re-myelination of the compressed focal segment will follow, leading to complete clinical and electrophysiological recovery.
Conclusion
Pregnancy-related carpal tunnel syndrome is not always a mild, chronic slowing of the median nerve. As demonstrated in this case, it can present with a subacute onset and a profound sensory conduction block.
For residents and practitioners in clinical neurophysiology, this case underscores the importance of segmental stimulation (palm-to-wrist). Unmasking a conduction block prevents the over-diagnosis of axonal loss, perfectly aligns with the pathophysiology of acute pregnancy-induced edema, and allows the clinician to confidently predict a full, reversible recovery.
References
Preston DC, Shapiro BE. Electromyography and Neuromuscular Disorders: Clinical-Electrophysiologic Correlations.
Kimura J. Electrodiagnosis in Diseases of Nerve and Muscle: Principles and Practice.
Dr. Abdelhamid NAILI, MD | Neuromedhub Lead Editor > Dr. Abdelhamid NAILI is a physician with a specialized focus in complex neuromuscular pathology and clinical neurophysiology (EMG). With extensive experience in hospital-based neurological services, his expertise lies in bridging the gap between theoretical neurophysiology and real-world clinical application. He is dedicated to advancing medical education through high-fidelity, case-based teaching.